
|
|
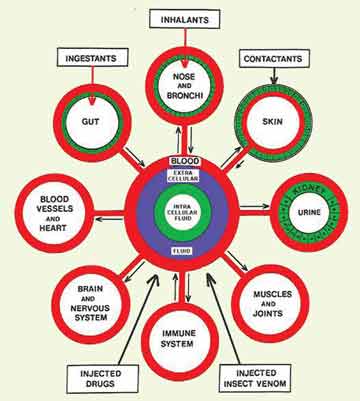
A guide to self-diagnosis of allergy or intolerance to food |
Dr Harry Morrow-Brown has practised as an allergist for over 50 years but despite the best efforts of a dedicated few, he believes that the provision for investigation into allergy in the UK remains ‘the most inadequate in Europe’. |
In Britain today allergies are suppressed with drugs as far as possible, doctors know little or nothing about them, and provision for investigation is the most inadequate in Europe. But there is nothing to prevent a patient trying to understand their allergies and attempt a self-diagnosis, so the following explanations and information may be helpful.
Anaphylactic shock Seasonal allergies Dust mites Also see Dr Morrow Brown's site at www.allergiesexplained.com First published in 2008 More articles on allergy testing
|












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}