
|
|
The cow and the coronary We normally worry about cow's milk in the context of cow's milk allergy or lactose intolerance but Margaret Moss suggests that its ingestion could have other long-term health consequences of which we should be aware. |
So somehow we have to eat, but preferably wholesome food that will sustain us through a long healthy life. The problem is how to discover what that wholesome food should be. Most medical research is about drugs, for the simple reason that drug companies have to test their wares before being allowed to sell them. They do randomised controlled trials. The idea is to have two groups of similar people, and to try the drug on one group, but not on the other group. This group is given a placebo, a pill that seems just like the drug pill, but that does not contain any of the drug. If the drug group does better than the placebo group, the drug must be better, mustn’t it? Well no, because the trial is often on people with just one problem, and then it is given to people with lots of problems. The volunteers for the trial are people who cope well with drugs. Drug sensitive people aren’t going to volunteer. Then the trial is brief, but the drug is given for many years. Drugs are tested on one group of people, perhaps men and women in their prime. They are then supplied to old people and children. Then companies paying for trials on their products tend to obtain better results than when testing is independent. I wonder why. Such randomised controlled trials are not possible for finding out what food causes death decades later. Who would volunteer to be part of a thirty year trial, where one half of the people ate sugar, and the other group ate something that looked and tasted the same, and no one knew which was which? Even if the groups did differently, it might be that sugar had a problem, or maybe the pretend sugar had some sort of effect on the body itself. Alternatively we might do experiments on rats, rabbits or mice, but they have different genes from us. Rabbits cannot handle cholesterol like we do. Rats can make vitamin C. We can’t. It would be expensive to run a large trial, and to analyse the food diaries of everyone who participates. One cheaper method that is sometimes tried involves asking people questions like, “How often do you eat a 100g piece of red meat?”, or “How much milk do you have in drinks and on cereal?” The questions are often unclear. What do you say, if you sometimes have 50g of ham in a sandwich, and other times have a 150g steak? What if you don’t like cereal and only drink fizzy drinks, but have lots of milk in instant mashed potato, custard tarts, packet soups, vodka and rice pudding? Anyway, do people remember exactly what they eat and drink, and does knowing that you have to fill in a form alter your behaviour? When researchers have compared the information people give in food diaries, with their responses to questions about how often or how much they eat a particular food, there is not much agreement. Because of the difficulty of doing research on food, the results are contradictory. People are fed up of reading today that coffee is bad for you and tomorrow that it is good. Some foods are good in one way, but bad in another. Some sources of alcohol may help our arteries, but alcohol is not good for the liver. Some of us therefore look at comparative figures of food consumption in different countries and at different times. We look at associations between food intake and later death from particular diseases. It is not a perfect technique, as it is possible that the people who died from the disease did not have a diet typical of their community. It may be that those who develop a fairly rare condition, like multiple sclerosis, have not followed a diet typical of their compatriots. When it comes to a common killer, like coronary heart disease, it is not plausible that such a large number of people have a diet very different from that of the average in their community. One thing to remember is that, if you are studying a disease that takes decades to kill, then you need to look at food intake years before death. You usually die of what you have been eating over many years, rather than of the current fashion at the time you die. We looked at food intake in 1971 and death seventeen years later from coronary heart disease in Organisation of Economic Cooperation and Development countries. Correlation is the statistical term used when we calculate an association between two things, like a food that is eaten, and the rate of death. Correlations are between -1 and +1. A correlation of 0 means there is no association. A positive correlation means that the higher one thing is, the higher the other is too. For example, maths and physics test results are positively correlated. Someone who is good at one is fairly likely to be good at the other. A negative correlation means that the higher one thing is, the lower the other. For example, the more exercise you take, the less likely you are to die of heart disease.
Milk 0.9 We found similar results for different age groups, and for women. If cholesterol and saturated fats were really the villains we have been told, would we find slight correlations of 0.2 and -0.1 for eggs and cheese? I doubt it. However, it is hard to believe that the very high correlation of 0.9 between milk consumption and coronary death occurs just by chance. If it is not the fat or cholesterol that is to blame, could it be the sugar? Milk contains lactose, a double sugar that splits into glucose and galactose in the body. This attaches to cholesterol, making it more likely to be deposited in artery walls, making arteries narrow. There is also a substance in cream, that has been shown in test tubes to clot human blood. The fairly high correlation with sugar, or sucrose, makes some sense too, as sucrose splits into fructose and glucose, which attach to cholesterol, causing deposits in artery walls. Again, it seems unlikely that the high negative correlations of vegetables and wine with coronary death are just due to chance. We know that purple grapes, like bilberries and blueberries, contain helpful antioxidants, and these end up in red wine. Magnesium reduces blood clotting. We know that vegetables provide magnesium, and antioxidants that are helpful to the arteries. Why does fruit score less well than vegetables? Because it contains more harmful sugar, and less magnesium than vegetables. Why does cheese show no connection with coronary death? Because the sugar is removed in the whey. Hard cheese is best, as it is pressed, to remove more whey. Cottage cheese is less good. Is there other evidence implicating the sugar in milk? Yes indeed. Different animals provide different milk. People in areas where the milk contains a lot of fat, but little sugar have low rates of coronary death. People in areas with low fat but high sugar milk have high coronary death rates. We also showed that European countries which reduced their milk consumption reduced their coronary death rates, while the Portugese increased their milk consumption, and the coronary rate went up. In Britain, milk consumption dropped in the late 1970s, coronary deaths in men and women dropping about ten years later. Before refrigeration, fermentation was a way of preserving food and drink. Fruit juice was fermented into wine, and milk into cheese. Countries where lactose intolerance is common tend to have low levels of coronary disease, because people either ferment the milk, or avoid having much of it. We don’t need milk for calcium. It is safer to obtain it from cheese. If you doubt that milk is connected with coronary heart disease, look at this table:
I calculated that countries consuming nearly one and a half times as much wine as milk minimise their coronary deaths. Perhaps the supermarkets should pack each 500ml of milk with a 750ml bottle of wine, as an antidote. Perhaps the milkman should only supply a bottle of milk together with a bag of vegetables, to antidote it. Alcohol damages the liver. So vegetables are a healthier option. It is important that those of us with food allergies and sensitivities avoid foods that make us ill. It is important however, to look at long-term health as well. The saturated fat and cholesterol hypotheses have benefitted the drug, margarine and sugar industries. Drug companies sell statin drugs, with harmful side effects. Food companies sell margarine, which may contain hydrogenated oil or harmful additives. Low fat food is often full of sugar, to make it palatable. I suggest eating cheese and butter rather than milk, having more vegetables than fruit, and avoiding cane and beet sugar, high fructose corn syrup and hydrogenated oil, if we want to care for our arteries. Margaret Moss
Click here for more research on cow's milk allergy First published in September 2012 |
 Food and drink kill. Occasionally someone eats food with a trace of peanut on, and dies rapidly of anaphylactic shock. It doesn’t happen often, but rare events are newsworthy, and we hear of it. Alcohol, of course, kills, after the drinker pilots a plane, drives a train, or car, or operates machinery. Hydrogenated oil, sugar and high fructose corn syrup kill, by increasing deaths from cancer and heart disease. Food contaminated with cholera, dysentery or typhoid kills, sometimes in large numbers. Unfortunately lack of food kills too. In a famine, the body uses up its deposits of fat, and then the immune system cannot mount an attack on infectious organisms. It appears that lack of vitamin D in food or from the sun leads to cancer, heart disease, multiple sclerosis, allergy and infection. So vitamin D deficiency kills too.
Food and drink kill. Occasionally someone eats food with a trace of peanut on, and dies rapidly of anaphylactic shock. It doesn’t happen often, but rare events are newsworthy, and we hear of it. Alcohol, of course, kills, after the drinker pilots a plane, drives a train, or car, or operates machinery. Hydrogenated oil, sugar and high fructose corn syrup kill, by increasing deaths from cancer and heart disease. Food contaminated with cholera, dysentery or typhoid kills, sometimes in large numbers. Unfortunately lack of food kills too. In a famine, the body uses up its deposits of fat, and then the immune system cannot mount an attack on infectious organisms. It appears that lack of vitamin D in food or from the sun leads to cancer, heart disease, multiple sclerosis, allergy and infection. So vitamin D deficiency kills too. These are the correlations between foods and coronary heart disease death that we found, for men of between 64 and 75 years:
These are the correlations between foods and coronary heart disease death that we found, for men of between 64 and 75 years: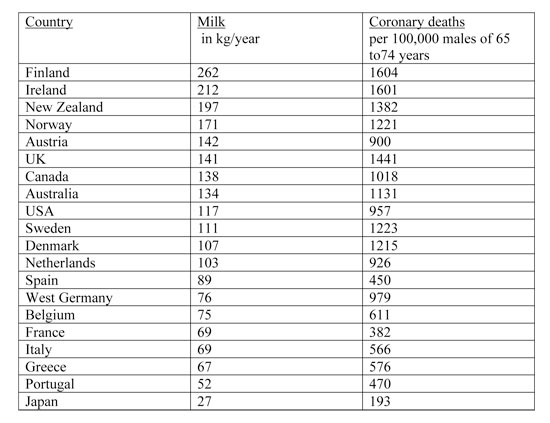












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}